Mainlined Science
Hi, all! Excited to see this community grow. Still figuring out Lemmy, so thanks for bearing with us. I want posts to have some form of identifier for ease in finding things so lets start every post with a tag before the title. Here are a few tag rules for now. **TAGS** - [QUESTION] - for posts directly asking input from the community. - [PAPER] - for posts about specific papers - [REVIEW] - for posts reviewing scientific literature, make sure to cite all papers discussed - [DISCUSSION] - for a more general post around any given topic or multiple topics **FORMAT**  If none of the tags seem to fit, a descriptive title will suffice. Thanks!

TLDR: wanna read a paper without the dumb publication house paywalls? Check out [Sci-Hub](https://en.wikipedia.org/wiki/Sci-Hub). Don't know how to properly read scientific literature? [Boom](https://www.docdroid.net/gEmWZcV/howtoreadpaper-pdf) This is mostly a PSA for the uninitiated, but you might find this useful. If nothing else I hope this is an enjoyable read to accompany you on the bus, at home, on the toilet, etc. One of the biggest hurdles in science is access to quality literature. Unfortunately, there are many roadblocks in place that prevent people from immediate entry to this material. Some journals frequently release free copies of their publications, but for the most part you need to be connected either through the academic field or by directly paying publishing companies. Paying is bullshit. This money does not go to the authors, and honestly, many of them will gladly give you copies of their published material if you ask. But if reaching out to random authors proves troublesome, you can always utilize [Sci-Hub](https://en.wikipedia.org/wiki/Sci-Hub). You'll notice that the link redirects to the wiki about Sci-Hub and the founder, Alexandra Elbakyan. The site domain changes often (which is why I didn't bother with a link) but with a little sleuthing you can find the most active and current iteration. This lovely site unlocks pay-walled scientific literature and provides you with a full text document that you can read in browser or save for later. One caveat is that it will be less reliable for current or new publications, they paused uploading new documents due to legal issues and it's unclear if they'll ever resume. Alright, next topic! **ReaDINg ComPReHenSIon** Still here? Oh, goodie! This isn't as boring as it sounds, but it also sorta is. Reading science papers is A LOT of work, like, a lot. But not for the reasons you might think. Yes, the material can be dense and seem completely undecipherable, but the biggest issues are sifting through the BULLSHIT. As you delve through the literature as a whole it's pretty clear that some papers are of a much higher quality than others. Why? Well, many reasons. Funding for the research, limitations in the researchers abilities to record quality data, and on and on. When I say BULLSHIT I don't mean that people are deliberately trying to put out false information, but poor data is a thing and it's out there. But I digress. Lets walk before we run. [Here is a lovely paper about how to read papers](https://dl.acm.org/doi/10.1145/1273445.1273458). You'll notice that it's pay-walled (womp womp) but lucky for you there's a way to get around that! I know, I'm making you work for it. If you don't want to test out Sci-Hub I did leave a direct link in the TLDR for ya. Anyway, this paper has a very simple and approachable method on how to digest lots of information. It does get a bit more intense near the end with most of the information targeted for individuals participating in research so don't despair on that front. I'll hop off my box for now. If you made it this far, thanks for reading! Looking forward to really getting into that good good niche research with y'all someday soon.
**Lipemia to Ketosis: A Historical Journey Through Fats in the Blood** Let’s take a deep dive into the world of fats in the blood, starting with the classic historical experiments on lipemia and ending with how ketosis and exogenous ketones fit into the picture of modern metabolic health. . ________________________________________ **Lipemia: The First Observations of Fat in the Blood** The story of lipemia—the condition where blood becomes milky or cloudy due to high levels of fat—begins in the early days of lipid metabolism research. Scientists noticed that after a fatty meal, blood drawn from patients sometimes had a creamy layer floating on top. This layer turned out to be chylomicrons, large fat particles that carry triglycerides (Fat molecules) from the intestines into the bloodstream after eating. In other cases, blood became uniformly turbid or milky—this was due to smaller fat particles (like VLDL and triglycerides) staying suspended in the liquid portion of the blood. These early observations of lipemia led to breakthroughs in understanding how fats travel through the body, why some people have abnormal lipid levels, and the role of these fats in metabolic disorders. ________________________________________ **Lipemia and Cardiovascular Risk: The Link to Atherosclerosis** From these early experiments, researchers learned that high triglycerides, the primary cause of lipemia, were linked to a higher risk of cardiovascular disease (CVD). When blood contains high levels of triglycerides, it also tends to carry more VLDL particles, which are rich in fats and cholesterol. Over time, this can contribute to plaque formation in the arteries. *LDL Oxidation and Foam Cells:* As LDL ("bad cholesterol") circulates through the blood, it can become oxidized, especially in people with elevated triglycerides or metabolic disorders. Oxidized LDL is engulfed by macrophages (immune cells) that turn into foam cells, which form the basis of atherosclerotic plaques. *Inflammation and Endothelial Dysfunction:* The accumulation of foam cells and fatty plaques in the arteries triggers inflammation, which further damages the arterial walls, eventually leading to the narrowing of blood vessels. This is the foundation of atherosclerosis, a key driver of heart attacks and strokes. ________________________________________ **Ketosis: The Body’s Natural Fat-Burning Mode** While lipemia deals with fats after digestion, ketosis is the body’s way of shifting to fat burning as a primary energy source. When carbohydrates are restricted, as in a keto diet or during fasting, the liver breaks down stored fat into fatty acids, which are converted into ketones. These ketone bodies (like beta-hydroxybutyrate) are then used as fuel in place of glucose. **The metabolic benefits of ketosis include:** *Fat loss:* By burning stored fat for energy, ketosis can lead to significant weight loss. *Lower triglycerides:* Over time, ketosis can reduce the amount of triglycerides in the blood, which helps improve cardiovascular health. (Caveat here is that post meal, which generally have a higher fat content for keto practitioners, levels will be transiently higher. Fasted blood monitoring is very important as will be discussed later.) *Improved insulin sensitivity:* Ketosis reduces the body’s reliance on glucose, which can enhance insulin sensitivity and help manage conditions like type 2 diabetes. ________________________________________ **Exogenous Ketones: The Shortcut, or Snake Oil?** Exogenous ketones are supplements that raise blood ketone levels without needing to follow a strict ketogenic diet. While they may temporarily increase ketones in the blood and provide a quick source of energy, the true metabolic benefits of ketosis—like fat loss and improved metabolism—come from the body producing its own ketones by breaking down stored fat. **Here’s the difference:** *What Exogenous Ketones Do:* They raise blood ketone levels quickly and may provide mental clarity or boost athletic performance--*in someone that needs an energy source!* **As in calories!!** If you are experiencing the “Keto crash,” exogenous ketones are useful in short bursts for quick energy while allowing you to remain compliant with your macros. *What They Don’t Do:* They don’t trigger the body to burn fat for fuel, so they don’t promote fat loss on their own. They don’t replicate the long-term benefits of being in natural ketosis, which is driven by metabolic changes like improved fat metabolism and lower insulin levels. While exogenous ketones can be useful for athletes or those in the keto trenches seeking a temporary cognitive respite from the keto fog, they’re often overmarketed as a way to achieve the benefits of ketosis without diet changes. I’m exercising a lot of restraint here cuz ya boi wants to go off! Can’t believe I managed to only imply that it is snake oil once in the title and then again here. That's it. Good job me! ________________________________________ **Connecting Lipemia, Ketosis, and Cardiovascular Health** At the intersection of lipemia and ketosis lies a key question: How do these metabolic processes influence cardiovascular risk? *Lipemia and CV Risk:* Elevated triglycerides, as seen in lipemia, are linked to a higher risk of atherosclerosis and cardiovascular events. When the blood is overloaded with fat, it contributes to plaque formation and arterial damage. *Ketosis and Lipid Profiles:* Natural ketosis, achieved through diet or fasting, can reduce triglycerides and potentially improve LDL/HDL ratios. However, some people may experience a rise in LDL cholesterol on a ketogenic diet, so it's important to monitor lipid levels carefully. ________________________________________ **In Summary:** Be safe out there y’all. I’m shouting these truths cuz I luv ya. No need to break your wallet with exogenous ketone products. Keto can be great for the right people but please be careful. Don’t get too comfortable out there with elevated lipids even if your doctor is ‘hip’ and says “we don’t really know long term effects of keto…” BAH! There is strong evidence for lipemia and cardiovascular risk, you know, heart attacks and strokes.. Take a statin or something. **With love,** InvolutedThymus ~XOXO
**Troponins: The Heart of Cardiac Diagnostics** Troponins are a big deal in medicine, especially when it comes to diagnosing heart attacks. Let's break down the basics of troponins, how they work in the body, and how we detect them in the lab. **What Are Troponins?** Troponins are proteins involved in muscle contraction, found in both skeletal and cardiac muscle. They’re part of the troponin-tropomyosin complex, which helps regulate muscle contraction by interacting with actin and myosin. There are three types of troponins: Troponin C (TnC) – Binds to calcium, triggering muscle contraction. Troponin I (TnI) – Inhibits muscle contraction in the absence of calcium. Troponin T (TnT) – Anchors the troponin complex to the muscle fiber. For cardiac diagnostics, we focus on cardiac-specific troponins: Troponin I (cTnI) and Troponin T (cTnT). These versions are unique to the heart muscle, making them incredibly important markers for detecting cardiac injury. When the heart is damaged, like during a heart attack, these cardiac-specific troponins are released into the bloodstream, signaling that heart cells are in distress. **Why Are Troponins Important?** Elevated troponin levels are a key indicator of myocardial injury (damage to the heart muscle), most often associated with acute coronary syndrome (ACS), which includes heart attacks. When heart cells are damaged due to ischemia (lack of oxygen), they break open, and troponins leak into the blood. Troponin tests are the gold standard for diagnosing heart attacks because they are sensitive (they detect even small amounts of damage) and specific (they’re associated with cardiac tissue, not other types of damage). This specificity is very important because in the ED a **panic attacks and even gastric reflux can present very similarly to heart attacks**. The lab is crucial to making sure we catch the cases that even the most experienced clinicians miss! **How Are Troponins Detected in the Lab?** The process of measuring troponins in the lab is highly standardized and involves several steps, starting with blood collection and ending with immunoassay analysis: Blood Collection and Processing: Troponin tests are typically done using either the green top (heparin) or lavender top (EDTA) tubes, depending on the lab. These tubes prevent blood from clotting, allowing for **plasma** testing. Which is faster than allowing the blood to clot (serum testing). Speed here is important for obvious reasons. (Technically both plasma and serum can and are used to measure troponins, but plasma testing is more common because it allows for quicker processing—there’s no need to wait for the blood to clot.) After collection, the sample is centrifuged to separate the plasma from the blood cells and transferred to a sample cup for testing by Immunoassay which involves specific antibodies designed to bind to cardiac-specific troponins (either cTnI or cTnT). When these antibodies bind to troponin in the blood sample, they trigger a signal (usually via chemiluminescence or fluorescence) that can be measured. The strength of the signal corresponds to the amount of troponin present in the blood. This value is then compared to a reference range. Each lab sets a reference range based on the assay, but in general, elevated levels of troponins suggest myocardial damage. The rise and fall pattern of troponin levels is key in diagnosing a heart attack—you’re not just looking for elevated levels, but how they change over time. Timing: Troponins typically rise within 3-6 hours after a cardiac event, peak at 12-24 hours, and can remain elevated for days. This pattern helps clinicians confirm the presence and extent of cardiac injury. **Other Markers for Myocardial Infarction** In addition to troponins, other markers may be measured for myocardial infarction (MI), though they’ve largely been replaced by troponins due to their higher sensitivity and specificity: *Creatine Kinase-MB (CK-MB):* CK-MB is an enzyme found in heart muscle and was used widely before troponins became standard. CK-MB rises and falls more quickly than troponins, which can be useful in detecting a reinfarction shortly after a heart attack. Many old school cardiologist swear by this marker! *Myoglobin:* Myoglobin is a small oxygen-binding protein that rises rapidly after muscle damage, but because it’s also found in skeletal muscle, it’s not specific to the heart. However, it can be an early marker for cardiac damage due to its rapid rise. *BNP/NT-proBNP:* These markers are released by the heart in response to **stretching** from heart **failure**. While not specific for heart attacks, elevated BNP levels can help differentiate between heart failure and other causes of similar symptoms, such as shortness of breath. More on this in a future post! Feel free to drop any questions or thoughts below! Let’s chat about how these tests have changed modern cardiology and what’s next in cardiac biomarker research!
**Why the Interventions Testing Program (ITP) Is the Gold Standard for Longevity Research** https://www.nia.nih.gov/research/dab/interventions-testing-program-itp/supported-interventions If you’re following the latest trends in longevity research, you’ve probably heard about a few "miracle compounds" like metformin, resveratrol, and NAD boosters. But let’s get real—when it comes to real preclinical data that actually holds up, nothing beats the Interventions Testing Program (ITP). And no, we’re not here to play along with the hype around these compounds that often don’t deliver in the lab. What Is the ITP and **Why Should You Care**? The Interventions Testing Program (ITP), run by the National Institute on Aging (NIA), is a uniquely well-designed testing platform that focuses on evaluating the effects of different compounds on lifespan and healthspan in **outbred** mice (meaning they have genetic diversity more like human populations, unlike the typical inbred strains). This gives the data more translational potential—interventions likely to work in humans are more likely to show efficacy in these outbred, well-powered experiments. This means the results aren’t confined to niche genetic conditions. The studies are conducted across multiple independent sites to ensure reproducibility and robustness of the data. Large sample sizes and rigorous methodology make this program a powerhouse for reliable preclinical results. If an intervention can work here, especially across different sites and genetically diverse mice, it’s hitting on something fundamental, not just a quirk of a specific strain or environment. **Metformin, Resveratrol, and NAD: Why We’re Not Impressed** Let’s get into why some of these so-called longevity wonder drugs don’t quite live up to their reputations: Metformin: While metformin has shown promise for managing glucose levels in type 2 diabetes, the data for longevity just doesn’t hold up. Large human clinical studies have failed to show any clear lifespan-extending benefits in healthy individuals. The ITP didn’t find significant longevity effects either, so while it’s a great tool for diabetes management, it’s not the fountain of youth people hoped for. Move on former mentor of mine I won't be naming.. move on.. Resveratrol: Remember when resveratrol was the darling of longevity science? With its *cough* "**too-good-to-be-true**" lab data, it got people excited about its potential anti-aging properties—until the ITP results showed no significant impact on lifespan... And labs that weren't financially invested didn't show impact on lifespan... And then the original lab results were shown to be a bit **too** nice… and then... Ya, it's all BS. Go check retraction watch or some other forum that hunts for data manipulation. The Red flags are R-E-D and its not from a wine stain... NAD Boosters: NAD boosters are the latest fad, but here’s where it gets funny: the same people (**person**... but let's say "people" for legal reasons) behind resveratrol are now pushing NAD as the next big thing. Fool me once with resveratrol, fool me twice with NAD? The ITP currently hasn’t looked at any NAD boosters other than Nicotinamide Riboside (NR) but that showed no impact and operates in the same pathway as NMN and NAD. I won't be holding my breath. Until compelling work of ITP caliber shows that boosting NAD+ levels leads to a longer life, it’s best to be skeptical until more solid data emerges. Rapamycin and Acarbose: **The True Stars of the ITP** Now let’s talk about the real heroes of the ITP: rapamycin and acarbose. These are the compounds you should be hyped about, and the data to back it up is strong. **Rapamycin**: If there’s one compound that’s consistently shown to extend lifespan, it’s rapamycin. Rapamycin works by inhibiting the mTOR pathway, which is a core regulator of growth, metabolism, and aging. What’s exciting about rapamycin is that it works not just in mice, but across a broad range of organisms—C. elegans, fruit flies, yeast, and even mammals. This isn’t some niche treatment that only works in tightly controlled conditions—it targets a fundamental mechanism in aging. It’s the real deal. **Acarbose**: Often overshadowed by rapamycin, acarbose has also shown significant lifespan extension in the ITP, especially in male mice. Acarbose works by slowing carbohydrate digestion and preventing large post-meal glucose spikes. And here’s the kicker: rapamycin and acarbose seem to work synergistically—they’re even more effective together than they are alone, suggesting they target different but complementary pathways involved in aging and metabolism. Both these drugs have shown impressive lifespan extension through the ITP and they play together nicely as well! See here: https://pubmed.ncbi.nlm.nih.gov/36179270/. Anyway, cool list of drugs right? Anything on the in process list that catches you eye? Any surprises revelations? What should be next?
I got into an interesting discussion at work about an MRI sequence I've never used before. For context, I did a bunch of brain imaging in grad school, and now at work I'm encountering things that aren't the brain. Shocking. The technique in question is trying to look at the amount of cartilage in a joint. I assumed the best way to identify potential problems with the MRI is to use a phantom like this one: https://www.truephantom.com/product/adult-knee/. We did this in grad school, but our phantom was basically an expensive jug of fancy water, which, apparently, looks enough like a brain to calibrate the machine. It turns out the hospital just takes a random resident, puts them in the MRI, and takes MRIs of their joints. I'm assuming it's because the hospital doesn't want to pay $10k for a fancy fake knee. So now I'm curious, if the radiologists and radiology-adjacent folks are out there, how many different phantoms do your teams own?
Let’s Talk Blood Collection Tubes and What the Colors Mean! Ever wonder what those different colored tops on blood collection tubes actually mean? Each color tells us something important about what’s inside the tube and how the blood will be processed. Let’s break it down, adding some cool science along the way! **Red Top** – No Additive Your blood is your blood! This tube contains no additives. A key property of blood is clotting—when exposed to air (more accurately activating factors), blood naturally forms a clot as platelets and clotting factors work to seal off a wound. In the lab, we let this clotting happen. As the blood clots, it traps certain components, like cells and proteins, forming a pellet. What’s left behind is serum, which is the liquid portion of blood without cells or clotting factors. This is used for tests like liver function or kidney panels where serum chemistry is important. **Gold or Tiger Top (SST)** – Serum Separator Tube Think of this as “Red with a plug!” This tube has a gel that sits between the clot and the serum after spinning the sample in a centrifuge. The gel forms a barrier, making it easier for lab techs to separate serum from the clot—no extra pipetting required. It’s a time-saver in the lab, used for tests similar to those with the red top. **Light Blue Top** – Sodium Citrate This tube stops clotting by binding calcium, a key player in the clotting cascade. Without calcium, the cascade can’t complete, so the blood remains unclotted. This is crucial for coagulation studies, like PT/INR (Prothrombin Time/International Normalized Ratio) and aPTT (Activated Partial Thromboplastin Time), which measure how well your blood is clotting. These tests are essential for monitoring patients on blood thinners or those with clotting disorders. The light blue tube is all about studying the clotting process without letting it happen in the tube. **Lavender or Purple Top** – EDTA (Ethylenediaminetetraacetic acid) EDTA works similarly to sodium citrate by binding calcium, but it’s used for a different purpose. While citrate prevents clotting for coagulation tests, EDTA is perfect for preserving the shape of blood cells. This makes it essential for tests like Complete Blood Counts (CBCs), where we’re looking at the size, shape, and number of blood cells under a microscope. EDTA doesn’t alter the cells, allowing for accurate analysis, whereas citrate is mainly interested in the clotting factors themselves. **Gray Top** – Sodium Fluoride/Potassium Oxalate Here’s where we get a bit more technical. This tube contains sodium fluoride, which inhibits enolase—a key enzyme in glycolysis, the process by which cells break down glucose for energy. Following Le Chatelier's principle, by blocking enolase, the reaction shifts away from breaking down glucose, keeping it stable for measurement. This is why the gray top is used for glucose testing. It also contains potassium oxalate, which further prevents clotting. Additionally, it’s often used for lactate testing, important for understanding conditions like sepsis. **Light Yellow Top** – ACD (Acid Citrate Dextrose) This one’s a bit more niche but fascinating. ACD is used in blood banking, especially for DNA testing or preserving blood for extended periods. The citrate prevents clotting by binding calcium, and the dextrose acts as a sugar source to keep the cells happy and viable for a longer shelf life. In donated blood, this mix helps preserve the cells for several weeks, making it critical for blood storage and transfusion medicine. **Pink Top** – EDTA (Like Lavender) You might wonder why we have pink when we already have lavender. Pink tops are specifically designated for blood banking, like crossmatches and blood typing. While it uses the same EDTA as lavender, the different color coding helps labs differentiate between general hematology tests (lavender) and blood banking tests (pink), ensuring the right sample goes to the right department. **Dark Blue (Royal Blue) Top** – Trace Element-Free This tube is special because it’s trace element-free. The tube itself is rigorously cleaned and prepared to avoid contamination from metals like zinc, copper, or lead. This is critical when testing for trace elements, where even a tiny contamination from the tube could alter the results. Some versions have EDTA, while others are additive-free, depending on the test being performed. **Black Top** – Sodium Citrate (Like Light Blue) Similar to the light blue top, this tube also contains sodium citrate, but with a different citrate-to-blood ratio. It’s used for the ESR (Erythrocyte Sedimentation Rate) test, which measures how quickly red blood cells settle in a test tube over an hour. ESR can give clues about inflammation in the body, making it useful for diagnosing conditions like autoimmune disorders or infections. The black top tube’s ratio is optimized for the slow sedimentation process. **Orange Top** – Thrombin This tube contains thrombin, a clotting agent that accelerates the clotting process. It’s used when you need serum quickly for emergency chemistry tests, like in the case of urgent cardiac enzyme tests. The thrombin speeds up the clot formation so the serum can be separated faster than in a red or gold top tube. **Green Top** – Heparin This guy contains heparin, an anticoagulant that prevents clotting by inhibiting thrombin and other clotting factors. This tube is used for plasma testing in clinical chemistry labs, especially for tests like electrolytes, ammonia, and troponins. Heparinized plasma allows for quicker processing because the blood doesn’t need to clot before being tested, making it ideal for urgent tests, such as when ruling out acute myocardial infarction (MI). **Serum vs. Plasma** - a reCAP Serum is the liquid portion of blood after it has clotted. When blood clots, the cells and clotting factors form a clot, leaving behind a clearer liquid—serum. This is what you get in tubes like the red or gold top (with no additives or a serum separator). Serum contains everything plasma does except the clotting factors, which are trapped in the clot. It’s often used for chemistry panels or hormone tests. Plasma is the liquid portion of blood before clotting. It’s what you get when you use tubes like the green top (heparin) or lavender top (EDTA) that prevent blood from clotting. Plasma contains water, proteins, electrolytes, hormones, and clotting factors (because the blood hasn’t clotted yet). It’s ideal for tests where you need to measure things like troponins or electrolytes quickly since the sample doesn’t need to clot first. And there you have it—a breakdown of the colorful world of blood collection tubes and their specific uses. The next time you’re in a lab or having blood drawn, you’ll know exactly what those tubes are doing and why they’re so important! Have any other lab-related questions? Let’s chat about them below!
Longevity and lifespan are a real hot topic right now. The amount of interest in the field has been increasing significantly and several labs are cranking out exciting new research. However, there is a lot of data out there and it can be tricky to interpret promising data from the noise. In response to this, a few researchers came together and put out a preprint on how to best gauge the quality of longevity interventions. https://www.sciencedirect.com/science/article/abs/pii/S1568163724003301 They argue in favor of choosing long lived controls, in this case lab mice, as a better marker for the robustness of any longevity intervention and state… “In the absence of independent replication, a putative mouse longevity intervention should only be considered with high confidence when control lifespans are close to 900 days or if the final lifespan of the treated group is considerably above 900 days.” This is the 900-day rule. Now, why is this important? Many studies in longevity research around mouse models use a variety of lab strains, and their median lifespans can differ dramatically. Let's say we have two studies, one has an intervention that is able to increase lifespan by 12% (intervention A) and the other shows a whopping 30% increase (intervention B) in lifespan. Which of these two sounds more interesting, more exciting, more desirable? In most cases that 30% increase is going to generate a lot of discussion and excitement, more so than a measly 12% lifespan bump. Details are key, and in this case the details are the longevity curves. I just said details are key, but I’m going to gloss over A LOT of information and just focus on longevity curves and median lifespans from a few different papers just to help illustrate this point. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9171804/ This study looks at gene therapy (and was mentioned in another post here) and boasts that “...mouse lifespan was increased up to 41%...” 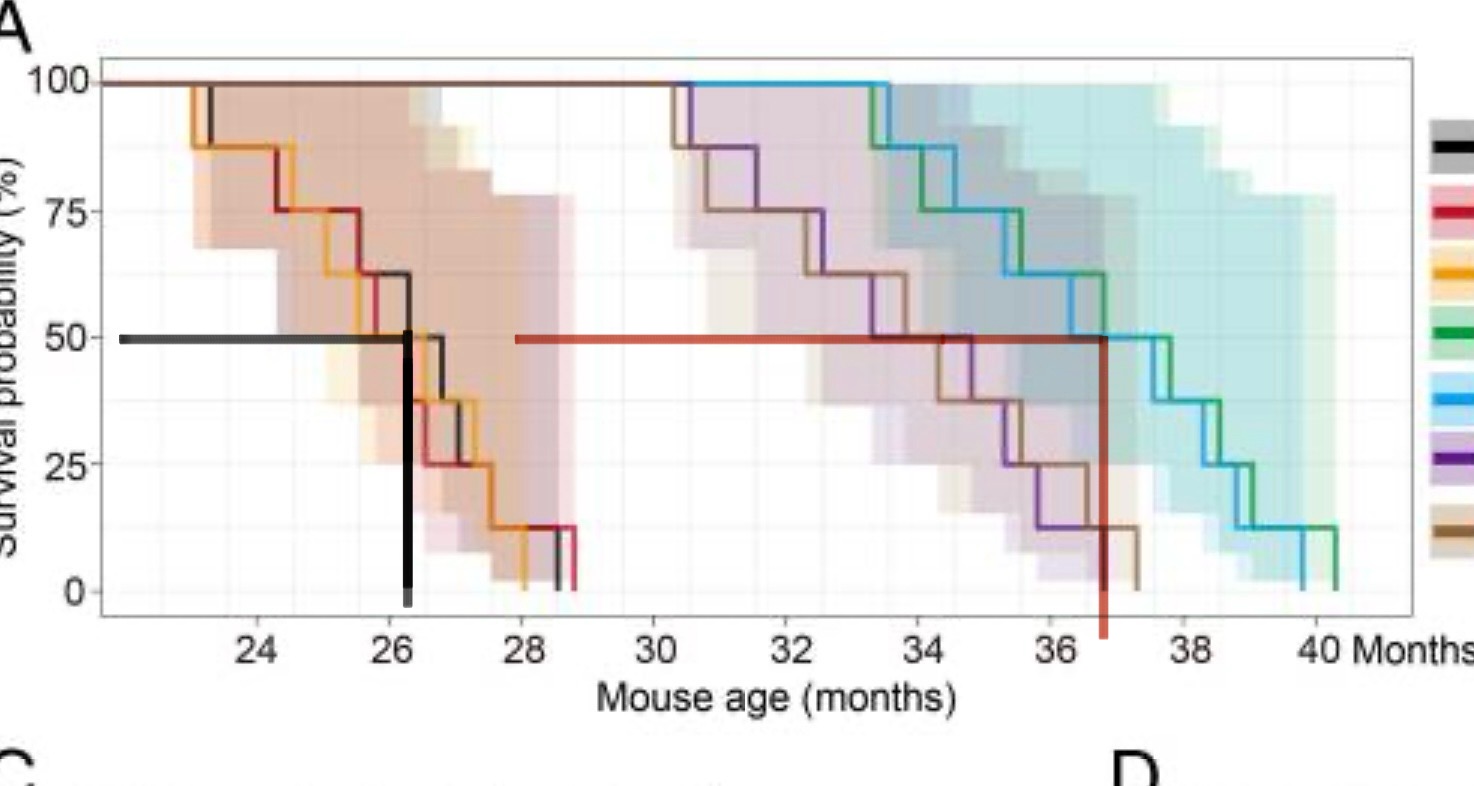 I’ve included their longevity curve and have added my own lines to help illustrate this, in black I’ve plotted the median lifespan of the control group, and red is median lifespan of the longest lived intervention group. We can easily see that the lifespan increase is significant, but does it pass the 900-day rule? The controls averaged just over 26 months, let's say approximately 790 days. Definitely under 900 days, barely hitting 800. So far it doesn’t quite make the grade. Let’s look at another paper. https://elifesciences.org/articles/16351 This one tested lifespan changes with rapamycin. There were multiple interventions, for now I’m just looking at one figure, longevity of the male cohort with ramapycin injections. 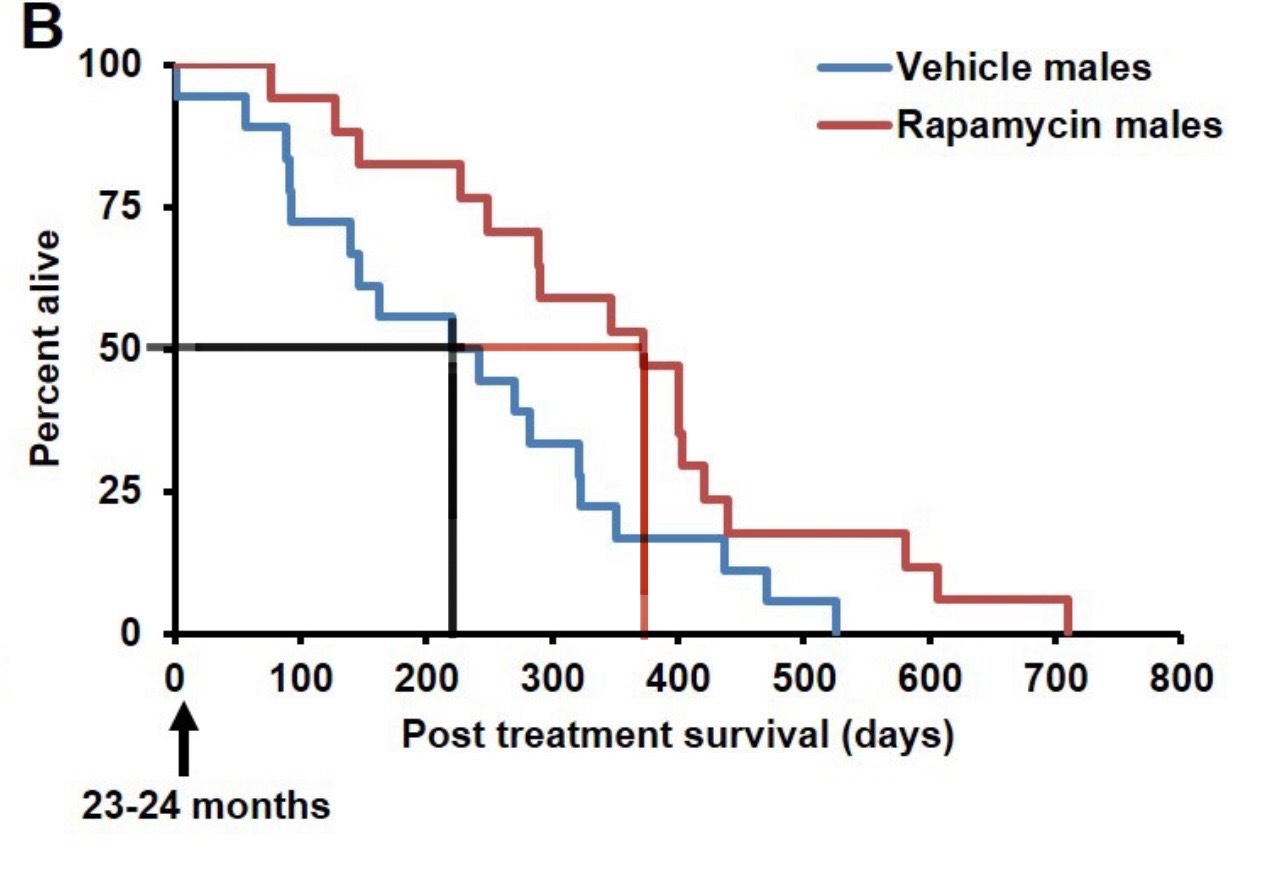 Once again I’ve plotted the median lifespan on the controls and intervention. We can already see the stark difference compared to the first paper. This lifespan bump looks pretty small by comparison, but let's look at the 900-day rule. Controls lasted on average a little over 200 days past 24 months, approximately 920 days. This is a long lived control. So, why is this important? If we can set a standard for longevity trials to only use long lived controls it significantly helps quantify the data as a whole. If you were quickly pursuing these papers, the takeaway might be that rapamycin is an inferior treatment compared to the gene therapy Jaiyan et al. tested. If nothing else the 900-day rule is the ultimate hype tester. I want to see exciting data showing lifespan increases as much as these researchers do, but be wary of the hype.
Full disclosure, this is outside my area of expertise (whatever that means…). I want to talk about the thymus and its importance in aging. I recently came across a fascinating paper that builds on a model of human lymphopoiesis across development and aging, and I wanted to share it with you all: (https://pubmed.ncbi.nlm.nih.gov/38908962). The thymus plays a key role in the immune system, especially in the production and maturation of T-cells, which are crucial for immune responses. One of the things that really piqued my interest is how the paper discusses developmental transitions in the thymus and how these changes potentially affect the immune system throughout life. It’s especially interesting how thymic involution with age may impact immune health, and how this could tie into the overall aging process. To me, it's wild that the thymus pretty much "dies" before we’re even out of our teens... Seriously, look at Figure 5. This idea has kept me up at night for about a decade now. Anyway, I’m in a transition phase of my career and am fortunate enough to have the latitude to start thinking deeply about the thymus. So let’s chat—we can struggle through my learning phase together! While I’m still learning the specifics, this got me thinking about the potential implications for therapies aimed at rejuvenating or maintaining thymic function in older individuals. Could these interventions help us preserve immune function as we age? You ever hear of this guy Greg Fahy? Interesting person. He has a fascinating publication history in the area of cryopreservation (another field I want to dive into, and we should totally discuss), but he’s also attempting to rejuvenate the thymus. Here’s one of his papers: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6826138. Honestly, I’m not sure where I stand on this yet. I find the hypothesis really interesting, but I’m in no way an immunologist. I’d love to hear your thoughts! If you’ve worked in this space or know of any relevant research, feel free to share. And if you haven’t but have a hot take, I’d love to hear that too! No barrier to entry—feel free to open this up. What areas in aging or immunology are you curious about? What do you think will get us to 130+ years on this planet!?
Hello Mainlined Science! We’re always looking for new topics and ideas to dive into, so we’d like to start getting some engagement! Got a question, a research area you’re curious about, or just something science-related that you’ve been pondering? Let’s talk about it! Even if it's outside our fields, no wrong answers! Whether it’s a specific field you want to explore or a “random thought of the day,” feel free to start up the chat, we will reply. We’re here to start discussions, share knowledge, and learn together. Drop your ideas below—there are also no wrong questions! I’m also thinking about occasionally hosting some hypothesis-generating sessions, starting small research projects, and maybe even setting up a little DIY lab. If there’s interest of course.. Maybe we could get into some 3D printing or simple bio experiments too! Let's see where this can go. Let's get the hive mind goin!
Ok, so I had a patient. The actual history isn't terribly important because this sort of thing happens relatively frequently, but to give you a quick one-liner: he was an older male with rheumatoid arthritis admitted for Staph bacteremia. In cases of blood infections, we order tests called "clearance cultures" to track and confirm that the organism we're fighting disappears with treatment. In this case, 1 out of 4 of these samples tested positive for a potential Bacillus species—the genus to which anthrax belongs. That being said, completely inert species of Bacillus are common contaminants in this setting, and the fact that only 1 out of 4 samples tested positive definitely makes you think this is such a case of contamination. However, we treat it as if it were anthrax until we're completely certain it isn't. It's Schrödinger's anthrax! After all, you don’t want to be the lab that missed anthrax. Bacillus anthracis Identification Colonies of B. anthracis appear non-hemolytic, consist of gram-variable rods with spore forms, and are non-motile. In other words, when grown on sheep's blood agar, they do not break down hemoglobin (a feature many microorganisms possess), appear elongated and purple or pink under a microscope after staining (gram-variable), produce spores (a survival mechanism), and lack motility (i.e., they don’t move via structures like flagella). We use these properties to rule out B. anthracis. While mass spectrometry is the gold standard for organism identification in modern microbiology, when it comes to potential anthrax, we revert to basic microbiological methods for safety reasons (which we can discuss more in the comments if you're interested). Bacillus anthracis: What Sets It Apart? Bacillus anthracis, the causative agent of anthrax, is a zoonotic disease, meaning it can be transmitted to humans through the handling or consumption of contaminated animal products. Due to its potential use as a bioweapon, B. anthracis is classified as a Tier I Category A agent by the CDC. Even though infection is rare in the United States, the micro lab remains vigilant in identifying this organism due to its serious implications. Plasmids and Virulence Factors What makes B. anthracis particularly dangerous are its virulence plasmids, pXO1 and pXO2, which carry the genes responsible for toxin production and capsule formation, respectively. These plasmids play a crucial role in the organism’s ability to cause disease, enabling it to evade the immune system and produce lethal toxins. But what exactly is a plasmid? What is a Plasmid? A plasmid is a small, circular piece of DNA that exists independently of the bacterial chromosome. Unlike the bacterial genome, which contains essential genes for the organism’s survival, plasmids often carry genes that provide advantages under certain conditions—such as antibiotic resistance or, in the case of B. anthracis, virulence factors. Plasmids are particularly interesting biologically and evolutionarily because they can be transferred between bacteria via a process called horizontal gene transfer. This means bacteria can acquire new traits, such as antibiotic resistance or enhanced pathogenicity, from other bacteria without evolving them slowly over generations. In essence, plasmids allow bacteria to adapt quickly to new challenges, making them highly versatile and resilient organisms. From an evolutionary standpoint, plasmids accelerate genetic diversity and adaptability, giving certain bacteria a survival edge in hostile environments. Think of it this way: plasmids let bacteria "plug and play" abilities. Imagine if I could transfer my height, immune system, or ability to play the ocarina just by touching you... now you're getting it. Because of these abilities plasmids are, in many ways, the cornerstone of modern biomedical tech. We will definitely be talking about them again. What is Bacillus cereus biovar anthracis and why use it to intro plasmids? Now, why bring up plasmids in this way? Because I can. Stories are nice. Anyway, plasmids are key to understanding another entity: Bacillus cereus biovar anthracis. This variant of B. cereus (the contaminant in our story) has acquired plasmids nearly identical to those found in B. anthracis, meaning it can cause anthrax-like diseases, particularly in animals. While B. cereus is more commonly known for causing food poisoning or being a random contaminant, its biovar anthracis variant is a real concern due to its ability to acquire these plasmids, making it capable of causing serious infections similar to anthrax. Mother nature is getting scarier! In 2016, this variant was added to the CDC’s select agent list, emphasizing the significance of monitoring its presence, especially in cases involving animals. Though not as common in humans, its existence underscores the evolutionary importance of plasmids in spreading virulence factors across bacterial species. Conclusion To wrap it up: Plasmids are fascinating, highly relevant to the changing landscape of infectious diseases, and, as will be discussed later, they might even change what it means to be human.
**What is Fasting and why do so many people seem to be into it?** There are many flavors of fasting, but they can be categorized into two main categories: intermittent fasting (IF) and time restricted eating (TRE). IF is defined as eating once every 24hrs and TRE is characterized by a shortened eating window, usually seen as 8hrs eating and 16hrs fasting. IF also know as one-meal-a-day (OMAD) and TRE have been farily popular over the last few years. They gained a lot of traction, almost a decade ago, with the hope that fasting mimicking diets could help with age related declines. The overall consensus now is that this type of fasting only imparts lifespan health benefits if you also restrict total calories. However, the hype was strong and most of these dietary methods are still championed today as a way to promote health. But can they actually provide any health benefit? Well, it depends. In the scope of nutrition and health, there's no better alternative than a well balanced diet. That being said, I think these interventions can be excellent tools for targeted goals i.e. weight loss/maintenance. Alright, this is gonna be real subjective, and your results may vary. Of course the metrics I'm most interested in might not apply to your desires or needs. For me, I prioritize dietary changes that can help me loose weight, primarily fat, quickly while maintaining as much lean mass as possible. Over the last 7 years I've dabbled with various dietary interventions, and here are my anecdotal results. **IF/OMAD** For me, IF has been the most effective tool for rapid weight loss, second only to prolonged fasting. As a rock climber it has been beneficial for me to apply a short stint of IF, 1-2 weeks, periodically when I'm trying to shed excess fat. Usually I resort to this type of eating after a multi month course of unchecked eating, especially when coming back from vacation. After some trial and error I learned that this can increase my chances for climbing injuries, and climbing after a few days of IF left me with really annoying achey fingers, primarily in my proximal and distal interphalangeal joints. Other activities were fine, such as hiking or mild resistance training. My takeaway is that IF is a very powerful tool for rapid weight loss, however, the potential for climbing related injuries makes it a short term success, but a long term failure. **TRE** Eating within time restricted windows is something my body has gravitated towards naturally. Growing up I was surrounded by people who were adamant about the importance of breakfast and I forced myself to eat in the mornings. This helped spark my hunger and after forcing down a small breakfast I would become ravenous 2 hours later. I now let my body choose and in the absence of food I really don't feel hungry until noon. So by default I mostly eat within an 8 hour window. This type of eating works well for me, but I wouldn't say it does anything special. However, this way of eating can help with weight maintenance. If you fall into the pattern of forcing down food every morning because you think you should, and your weight tends to fluctuate easily, this might be a beneficial diet. **Ketogenic Diets** Yes, this one is a wildcard. While this diet might not be recognized as a fasting intervention it does mimic fasts, since it puts your body into a state of ketosis, which is what fasting also does. Also, this is the one dietary intervention that has been consistently effective in helping me lose fat while maintaining, even gaining, muscle mass. I've had a lot of trial and error with this one too, and I've now come to prefer a more carb and protein friendly version that allows me to keep climbing at peak performance. Typically a keto diet is very low carb, modest protein and liberal fat. I prefer higher protein, aiming for 150g on a daily basis, and am not worried about gluconeogenesis, where dietary protein is converted to glucose. On a daily basis my carb intake is between 50g and 100g, depending on my activity levels. I eat a large amount of vegetables, including higher carb sources such as red bell pepper, squash and zucchini. With small amounts of fruit, usually blueberries or dried plums. My fat intake is tied into my protein intake as I prioritize beef over other forms of protein, but will cook vegetables in avocado oil. For me, this hybrid ketogenic diet has worked well. I'm still able to lose weight at a rate comparable to IF (not quite as potent), but am able to maintain athletic performance and keep climbing without injuries. However, this way of eating does come with risks, namely high cholesterol. I've attempted various modes of ketosis, and have played around with other sources of protein and fat, but so far it hasn't made a difference. After prolonged use (>1 month) my LDL rises dramatically. If I were using this diet long term I would utilize pharmaceuticals to get these levels under control, but in the interim I apply this diet briefly and very infrequently. I tend to slip into ketosis somewhat easily, but I'm not sure if this is something my body is naturally predisposed to or if my keto cycles have promoted this adaptation. My current protocol is to apply this diet for about 3 weeks at a time and I'll cycle this about 3-4 times a year depending on needs. Pros: fat loss, strength gains, higher perceived energy levels. Cons: high cholesterol, can't eat pie. So, those are my thoughts. But what do you think? Is there a dietary intervention that has been life-changing for you? Do you have any concerns with diets? Do tell!
OK, Time for Something Random: Lyme disease and its strange connection to lizards. Lyme disease is a big deal. Especially, or at least historically, here on the east coast US. Did you know that some animals can actually cure infected tick carriers!? I didn't either. In parts of California, western fence lizards play a surprising role in controlling Lyme disease. When ticks feed on these lizards, a protein in their blood kills the bacteria (Borrelia burgdorferi) that causes Lyme disease. Some factor in the lizards blood is ingested and kills the bacteria present in the gut of the tick. To conclude, nature is wild. Much of our innovation in biology/medicine, including CRISPR (see earlier related posts) and the majority of our antibiotics, aren't so much inventions but are more accurately 'discoveries.' Relevant papers I happened upon: https://pubmed.ncbi.nlm.nih.gov/9488334/ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5413869/
Let’s continue our dive into gene therapy with one of my favorite papers. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6876218/ In this study, researchers delivered three longevity-associated genes (FGF21, αKlotho, and sTGFβR2) to mice using a gene therapy cocktail. These genes target metabolism, heart function, and kidney health—three areas that typically decline with age. Here’s why this is a big deal: Obesity & Diabetes? Reversed. Mice fed a high-fat diet lost weight and saw their diabetes symptoms disappear, just by tweaking how their cells handled energy. Heart Failure? Improved. The therapy improved heart function by 58%, meaning it could help tackle the leading cause of death worldwide. Kidney Disease? Protected. Mice treated with this gene therapy avoided the typical kidney damage seen with age-related conditions. What’s most exciting is that a single gene therapy cocktail—combining just two of the three genes—was able to treat all of these diseases simultaneously. Imagine being able to tackle multiple age-related health issues with just one treatment! This approach could be a game-changer in how we think about aging and disease. Instead of targeting one condition at a time, we might be able to treat aging itself by addressing the root causes of multiple diseases. What do you think—are we on the verge of a breakthrough in how we fight age-related diseases? See this similar paper here targeting TERT and follistatin: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9171804/ Do these papers pass our threshold of believability? Are we concerned that one of these papers had a few post publication amendments? I may circle back to poke holes in them (if I can find any) at a later time. Feel free to beat me to it!
Let’s talk CRISPR-Cas9 and why it’s one of the most significant breakthroughs in modern biology. At its core, CRISPR-Cas9 is a tool for precise genome editing. Before CRISPR, genetic modification was a slow, expensive, and often imprecise process. CRISPR changed the game by allowing scientists to cut DNA at specific sites, guided by an RNA molecule that can be customized to target nearly any gene. Once the DNA is cut, it can be repaired in a way that adds, deletes, or alters the genetic sequence. This kind of precision has opened up endless possibilities. Why is this such a big deal? Speed and Efficiency: CRISPR allows scientists to make changes to the DNA of organisms in weeks, not years. You want to knock out a gene? You can do that. Want to introduce a new one? Done. The speed and flexibility are revolutionary compared to older methods. Precision: CRISPR can zero in on specific genes with high accuracy, reducing the risk of off-target effects (though this is still an area of research). Precision matters when you’re editing the building blocks of life. Wide Applications: It’s not just a tool for basic research—CRISPR is shaping medicine, agriculture, and even biotechnology. Scientists are working on curing genetic disorders, creating disease-resistant crops, and engineering cells to fight cancer. The potential here is massive. How is CRISPR shaping biology today? Gene Therapy: One of the most exciting applications is in treating genetic diseases like sickle cell anemia, muscular dystrophy, and certain forms of blindness. By directly editing the faulty genes responsible for these conditions, CRISPR could offer permanent cures rather than just treating symptoms. Cancer Research: CRISPR is being used to edit immune cells, making them better at recognizing and attacking cancer. We’re moving closer to personalized medicine where your immune system can be genetically fine-tuned to fight off specific diseases. Agriculture: In crops and livestock, CRISPR is being used to enhance yields, create resistance to pests and disease, and improve nutritional content. This could help address food security as populations grow and climates change. Basic Research: Perhaps one of its most profound impacts is that CRISPR makes it easier to explore how genes work. We’re learning more about gene functions at a faster pace than ever before, and this knowledge feeds into all other areas of biology. Of course, with great power comes great responsibility. There are ethical considerations around using CRISPR, especially when it comes to editing human embryos or making changes that can be passed down to future generations. The technology is advancing quickly, but society will need to decide how to handle the moral implications. In summary, CRISPR-Cas9 is a huge deal because it makes genome editing faster, cheaper, and more accurate than ever before. It’s shaping everything from how we fight diseases to how we grow food, and it’s rapidly transforming the future of biology. We’re just starting to scratch the surface of its potential. Suggested reading: The paper that started all https://pubmed.ncbi.nlm.nih.gov/22745249/ A look at a future where everyone has access to the power of CRISPR https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11297044/
This is a preprint, which means that the article has not been peer-reviewed yet. This is all part of the normal process, researchers will often present their findings before their work is published. Here the deets! The AgelessRx-sponsored Participatory Evaluation of Aging with Rapamycin for Longevity (PEARL) trial was a 48-week randomized, double-blind, placebo-controlled trial investigating the safety and potential efficacy of different intermittent rapamycin doses for mitigating signs of aging. More info! https://clinicaltrials.gov/study/NCT04488601 https://agelessrx.com/results-of-the-pearl-trial/